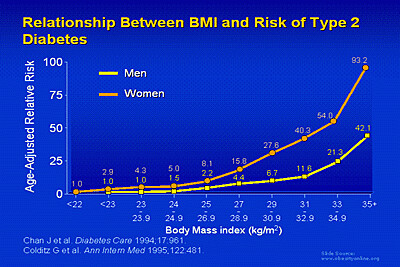
Before BMI standards were widely adopted in the 1980s, fatness was largely determined by height/weight charts. Those early BMI standards considered men with a BMI >=27.8 and women with a BMI >=27.3 to be "overweight." Then in 1998, the National Institutes of Health lowered their BMI cutoffs to match the World Health Organization standards. Under the new guidelines, a BMI of 25 or more was considered "overweight," and 30 or more was considered "obese." It sounds a little convenient that these categories happen to fit such nice round numbers, doesn't it? But this is pretty much the basis for these categories:
And also, to a lesser extent, this:
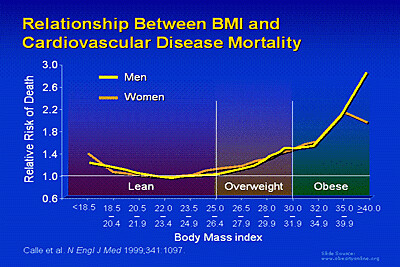
(These images courtesy of Obesity Online).
The relative risk of diabetes and heart disease goes up at a BMI of 25, and the line of BMI vs. risk seems to change slope at around BMI = 30 (references are on the images). And BMI is cheap and easy to measure, all you need is a scale and a yardstick, or even just a telephone--you can just do a survey and ask people their height and weight. In contrast, to actually measure fat mass accurately, you need a machine called a DEXA scanner which costs $20K-$80K depending on how fancy your machine is.
So those are the main reasons why BMI is so popular among researchers and clinicians. Now, on to the criticisms.
The main criticism I hear of BMI is that it is simply a height/weight ratio and does not take into account muscle mass. While this is true, most people (women especially) are not going to be much affected by this unless they are body builders or professional-caliber athletes. Take, for example, Cruiserweight boxing champion David Haye, pictured here:

A very muscular guy, obviously, yet his fighting weight BMI clocks in right at 25, the border between normal and overweight (he's 6'3" and the Cruiserweight limit is 200 lbs. I chose a boxer for this example, because I figure their weights must be pretty accurate). The point here being that while muscle mass is one of the more common criticisms people have of BMI, I think that for the most part it's not that big a confounding factor in most cases.
One element that does seem to be a major confounding factor is race. Several studies have shown that people of Asian descent tend to be fatter than Caucasians with the same BMI, and consequently, they tend to develop weight-related illnesses at lower BMIs (1-4). Latinos also seem to be more susceptible to diabetes at lower weights, although less so than Asians (4). For this reason, some people now think that waist circumference is a better indicator of risk of overweight-associated illness, and other researchers suggest that using the two measurements in tandem provides the best estimate of risk (5-7).
In addition to racial differences, some investigators feel that BMI cutoffs should be different for women and men, as men tend to have more muscle mass due to their higher testosterone levels. As you can see in the graphs above, men have a lower relative risk of diabetes vs. BMI compared to women, but the risks for cardiovascular disease are similar.
Another major problem with using BMI as a determinant of health risk is the fact that several recent studies have shown that people with overweight BMIs have a lower risk of mortality than people with normal BMIs (8-9). (Of course, everyone's risk of mortality is 100% eventually, but this was as measured within the period of the study). This finding was perplexing to researchers, as it would seem to counteract the information in the graphs above, findings which had been replicated many times. Some have suggested that these findings could be a result of some people in the "normal" group experiencing weight loss due to undiagnosed illness that later contributed to death. Others pointed to the so-called "obesity" paradox: the finding that while overweight people are more likely to be diagnosed with heart disease and renal failure, they also have a survival advantage over normal-weight people with this disease (10). (There's a lot more to say about the obesity paradox, but I'll save it for another post!) At any rate, the overall picture is still quite murky.
In summary, I would say that BMI is a somewhat useful tool for determining whether a person is statistically at heightened risk for certain complications of obesity. But it should be kept in mind that this increased probability is not at all a predetermined fate. After all, even a 45-year old woman with a BMI of 30-35 still has less than a 50% chance of developing type II diabetes (11). So, as they say on the internet, YMMV.
1. WHO Expert Consultation.
Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. The Lancet. 363: 157-163, 2004.
2. Deurenberg-Yap M., Deurenberg P. Is a re-evaluation of WHO body mass index cut-off values needed? The case of Asians in Singapore. Nutrition Reviews 61:S80-S87, 2003.3. Huxley R, James WP, Barzi F, Patel JV, Lear SA, Suriuawongpaisal P, Janus E, Caterson I, Zimmet P, Prabhakaran D, Reddy S, Woodward M, Obesity in Asia Collaboration. Ethnic comparisons of the cross-sectional relationships between measures of body size with diabetes and hypertension. Obesity Reviews 9:53-61, 2008.
4. Shai I, Jiang R, Manson JE, Stampfer MJ, Willett WC, Colditz GA, Hu FB. Ethnicity, obesity, and risk of type 2 diabetes in women: a 20-year follow-up study. Diabetes Care 29: 1585-1590, 2006.
5. McCarthy HD. Body fat measurements in children as predictors for the metabolic syndrome: focus on waist circumference. The Proceedings of the Nutrition Society 65: 385-392, 2006.
6. Deurenberg P, Deurenberg-Yap M. Validity of body composition methods across ethnic population groups. Forum of Nutrition 56: 299-301, 2003.
7. Koster A, Leitzmann MF, Schatzkin A, Mouw T, Adams KF, van Eijk JT, Hollenbeck AR, Harris TB. Waist Circumference and Mortality. American Journal of Epidemiology April 15 Epub ahead of print, 2008.
8. Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess deaths associated with underweight, overweight, and obesity. Journal of the American Medical Association 293: 1861-1867, 2005.
9. Flegal KM, Graubard BI, Williamson DF, Gail MH. Cause-specific excess deaths associated with underweight, overweight, and obesity. Journal of the American Medical Association 298: 2028-2037, 2007.
10. Schmidt DS, Salahudeen AK. Obesity-survival paradox--still a controversy? Seminars in Dialysis 20: 486-492, 2007.
11. Narayan KMV, Boyle JP, Thompson TJ, Gregg EW, Williamson DF. Effect of BMI on Lifetime Risk for Diabetes in the U.S. Diabetes Care 30: 1562, 1566, 2007.
